
“Will this ever go away?” It is the first question most women ask after a PCOS diagnosis — and one of the hardest to answer honestly. If you have spent any time searching online, you already know the chaos that awaits: miracle supplements, detox teas, Instagram wellness coaches promising to “reverse” your PCOS in 30 days, and contradictory advice that leaves you more confused than when you started. You deserve better than that. This blog cuts through the noise and gives you exactly what gynecologists, endocrinologists, and reproductive specialists actually say about PCOS, whether it is permanent, and what genuine, long-term PCOS management truly looks like.
What Is PCOS — And Why Is It So Complex?
Polycystic Ovary Syndrome is one of the most common hormonal conditions affecting women of reproductive age, yet it remains widely misunderstood — even within healthcare settings. Understanding its complexity is the first step to understanding why a simple cure remains out of reach.
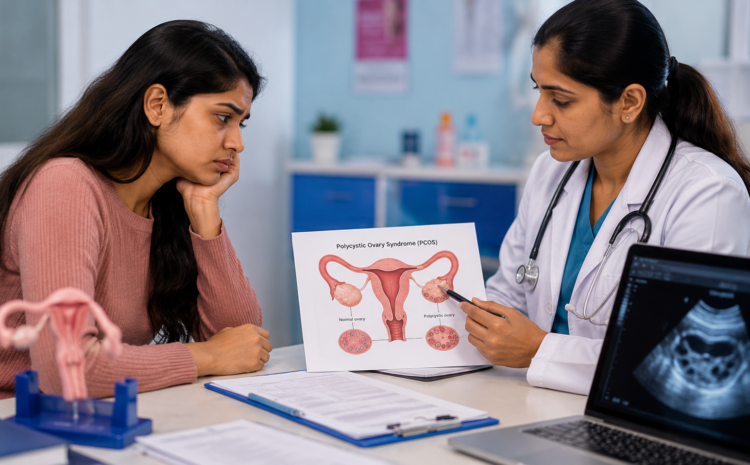
- PCOS stands for Polycystic Ovary Syndrome — a hormonal disorder characterised by elevated androgens (male hormones), irregular or absent ovulation, and in many cases, the appearance of small follicle cysts on the ovaries.
- PCOS is a syndrome, not a single disease, meaning it is defined by a cluster of symptoms rather than one identifiable cause, and no two women experience it in exactly the same way.
- The Rotterdam Consensus criteria — the internationally accepted diagnostic standard — requires that a woman meet at least two of three criteria: irregular or infrequent periods, clinical or biochemical signs of high androgens (such as acne, hair loss, or elevated testosterone), and polycystic ovarian morphology on ultrasound.
- PCOS presents across four recognised subtypes — lean PCOS, insulin-resistant PCOS, inflammatory PCOS, and adrenal PCOS — each with its own hormonal profile, triggers, and treatment priorities.
- This diversity is precisely why a one-size-fits-all cure is impossible. What works beautifully for one woman’s insulin-resistant PCOS may be entirely inadequate for another woman whose PCOS is driven by adrenal androgen excess.
The Honest Answer: Is There a Cure for PCOS?
No PCOS currently has no known permanent cure. However, it is one of the most highly manageable hormonal conditions in women’s medicine, and with the right interventions, many women achieve near-normal hormonal function and excellent quality of life.
- “No cure” in clinical terms means there is no single treatment, medication, or procedure that permanently eliminates the underlying hormonal dysregulation that defines PCOS — it cannot be surgically removed or resolved with a short course of tablets.
- PCOS is considered a lifelong hormonal condition because its root causes — genetic predisposition, insulin resistance, and hypothalamic-pituitary axis dysfunction — do not disappear with treatment, even when symptoms are fully controlled.
- Symptoms can and do go into remission with the right combination of lifestyle modifications, medical treatment, and ongoing monitoring, and many women experience long stretches where PCOS feels entirely absent from their lives.
- Managing a condition into near-normal function is not a consolation prize — it is the clinical goal for dozens of chronic conditions including thyroid disorders, type 2 diabetes, and hypertension, all of which are similarly “incurable” but routinely well-managed.
- Early diagnosis dramatically changes your long-term trajectory. Women who receive an accurate PCOS diagnosis early and begin appropriate PCOS management are far less likely to progress to type 2 diabetes, cardiovascular disease, or endometrial cancer than those who go undiagnosed for years.
What Doctors Actually Recommend Instead of a Cure
Lifestyle Modifications as First-Line Treatment
PCOS lifestyle changes are not optional add-ons — they are the foundation of every evidence-based management plan, recommended ahead of medication in most international clinical guidelines.
- An anti-inflammatory, low-glycemic diet helps reduce the chronic low-grade inflammation associated with PCOS and prevents the blood sugar spikes that worsen insulin resistance and androgen production.
- Regular aerobic and resistance exercise directly improves insulin sensitivity at the cellular level, which in turn lowers circulating androgens and can restore more regular ovulation.
- Even a 5–10% reduction in body weight in women with overweight-associated PCOS has been shown in clinical studies to restore ovulatory cycles, reduce androgen levels, and improve metabolic markers — without any medication.
- Sleep quality has a measurable hormonal impact — chronic sleep deprivation elevates cortisol and disrupts insulin regulation, making PCOS symptoms significantly harder to control.
- Stress management is a legitimate medical priority for women with PCOS, because chronically elevated cortisol stimulates adrenal androgen production and worsens the hormonal imbalances that drive symptoms.
Medical and Hormonal Treatments
When lifestyle modifications alone are insufficient — or when specific symptoms require targeted treatment — doctors have a well-established toolkit of PCOS hormonal treatments and medications.
- Combined oral contraceptive pills remain the most widely prescribed treatment for cycle regulation, reducing androgen levels and protecting the endometrial lining against the risks of chronic anovulation.
- Metformin, originally developed for type 2 diabetes, is frequently prescribed for insulin-resistant PCOS to improve cellular insulin response, lower circulating insulin, and in some cases, restore ovulation.
- Letrozole and clomiphene citrate are the gold-standard medications for ovulation induction in women with PCOS who are trying to conceive, with letrozole now preferred by most reproductive specialists.
- Spironolactone is an anti-androgen medication commonly prescribed for androgen-driven symptoms such as acne, hirsutism (unwanted hair growth), and female pattern hair loss.
- All treatment plans should be individualised — your PCOS subtype, your symptoms, your reproductive goals, your metabolic profile, and your personal preferences should all shape the specific combination of treatments your doctor recommends.
Emerging and Investigational Treatments
The science of PCOS treatment is advancing rapidly, and several emerging approaches show genuine clinical promise.
- Inositol supplementation — particularly the combination of myo-inositol and D-chiro-inositol — has growing research support for improving insulin sensitivity, restoring ovulation, and reducing androgen levels in women with PCOS.
- Gut microbiome research is revealing significant differences between the intestinal bacteria of women with and without PCOS, opening up potential future therapeutic pathways targeting the gut-hormone axis.
- eGLP-1 receptor agonists such as semaglutid are being actively investigated in PCOS populations, with early evidence suggesting meaningful improvements in weight, insulin resistance, androgen levels, and menstrual regularity.
- Multiple clinical trials are currently underway exploring new hormonal targets, novel anti-inflammatory agents, and precision medicine approaches that tailor PCOS treatment to a woman’s specific genetic and metabolic profile.
- The next decade of PCOS research is likely to produce significantly more targeted therapies — making it more important than ever to stay engaged with your healthcare team and not settle for outdated or inadequate management.
Common Myths About Curing PCOS — Debunked
- “Getting pregnant cures PCOS” is false — pregnancy temporarily suppresses some PCOS symptoms due to altered hormone levels, but the underlying condition persists after delivery, and symptoms typically return postpartum.
- “Losing weight will make PCOS disappear“ contains a grain of truth but misrepresents the reality — weight loss can dramatically improve symptoms and metabolic markers, but it does not eliminate the genetic and hormonal predisposition that causes PCOS.
- “Going off birth control means your PCOS is gone“ is one of the most common misconceptions — the pill masks PCOS symptoms rather than treating the underlying condition, so irregular periods, acne, and other symptoms frequently return when contraception is stopped.
- “Detox teas and supplements can reverse PCOS“ is not supported by any credible clinical evidence — many products marketed to PCOS sufferers online have no published trial data, and some contain ingredients that may interact with prescribed medications.
- “PCOS only matters if you want to get pregnant“ dangerously underestimates the condition — women with PCOS face significantly elevated lifetime risks of type 2 diabetes, cardiovascular disease, non-alcoholic fatty liver disease, and endometrial cancer, all of which require proactive monitoring regardless of reproductive goals.
Can PCOS Symptoms Improve Over Time?
Many women notice a genuine shift in their PCOS experience as they move through their 30s and 40s — and there is clinical evidence to support what they are observing.
- Androgen levels tend to decline naturally with age in women with PCOS, which is why symptoms like hirsutism and acne often become less severe in the decade before menopause.
- Menstrual cycles may become more regular in some women’s 30s and 40s as the hormonal fluctuations of the early reproductive years begin to stabilise.
- The approach of menopause brings its own hormonal shift that can further ease the reproductive symptoms of PCOS, though it does not eliminate the condition.
- Metabolic risks do not diminish with age — in fact, the risk of type 2 diabetes and cardiovascular disease increases as women with PCOS age, making ongoing monitoring non-negotiable even when you feel significantly better.
- Feeling better is not the same as being medically safe — regular blood glucose, lipid, and blood pressure checks remain essential throughout your life with PCOS, even during long periods of symptom remission.
PCOS Across Life Stages: What Changes and What Doesn’t
- In adolescence, PCOS is frequently missed or misdiagnosed because irregular periods are common in the early years after puberty, delaying diagnosis and early intervention.
- During the reproductive years, the focus of PCOS management typically centres on cycle regulation, fertility support, insulin resistance control, and androgen-related symptom management.
- Pregnancy with PCOS carries elevated risks of gestational diabetes, pregnancy-induced hypertension, and preterm birth — all of which require specialist monitoring and targeted antenatal care.
- In perimenopause, the hormonal transition can temporarily worsen some PCOS symptoms before the natural decline in androgen production brings partial relief.
- After menopause, the metabolic dimension of PCOS — insulin resistance, cardiovascular risk, and glucose regulation — becomes the primary focus of ongoing medical care and monitoring.
The Role of a Multidisciplinary Care Team
Living well with PCOS requires more than a single prescription from a single doctor — it requires a coordinated team of specialists who understand how the condition’s many dimensions interact.
- PCOS should never be managed by one clinician alone, because its hormonal, metabolic, reproductive, dermatological, and psychological dimensions each require specific expertise.
- The ideal PCOS care team includes a gynaecologist or reproductive endocrinologist, a general endocrinologist, a registered dietitian with experience in hormonal health, a dermatologist for skin and hair concerns, and a mental health professional to address the significant psychological burden PCOS often carries.
- Coordinated care consistently produces better outcomes — women whose PCOS is managed collaboratively experience faster symptom resolution, lower rates of metabolic complications, and significantly higher quality of life.
- Regular monitoring of blood glucose, HbA1c, lipid panels, blood pressure, and reproductive hormones is the clinical standard of care for PCOS and should be part of your annual health review regardless of how well your symptoms are controlled.
- Advocating for yourself in healthcare settings is essential — PCOS remains chronically underdiagnosed and undertreated, and you should feel empowered to request specialist referrals, second opinions, and comprehensive testing if your concerns are not being taken seriously.
Living Well With PCOS: A Long-Term Mindset Shift
- Reframe PCOS from a life sentence to a manageable condition — millions of women worldwide live full, active, fertile, and healthy lives with PCOS, and your diagnosis does not define the ceiling of what is possible for you.
- Build sustainable lifestyle habits rather than chasing quick fixes, because the women who manage PCOS most successfully over decades are those who make incremental, realistic changes — not those who attempt extreme interventions that collapse within weeks.
- PCOS communities — online and in person — offer genuine peer support from women who understand the frustration, grief, and determination that come with navigating this condition, and connecting with them can meaningfully reduce the isolation many women feel.
- Tracking your symptoms, cycles, energy levels, and skin changes keeps you informed, helps your doctor identify patterns, and gives you a sense of agency over a condition that can otherwise feel entirely out of your control.
- Celebrate every small win in your management journey — a more regular cycle, clearer skin, improved lab results, or simply more energy than last month are all meaningful victories worth acknowledging on the road toward a symptom-managed life.
Conclusion
PCOS may not have a cure yet — and that is a valid source of frustration, grief, and anger. Your feelings about that are completely legitimate. But here is what is equally true: PCOS is one of the most researched, most treatable, and most manageable hormonal conditions in women’s health today. The goal of PCOS management is not to wait passively for a cure that does not yet exist. It is to build a full, healthy, active life in which PCOS is a manageable background condition rather than a daily obstacle. That life is genuinely within reach. Book a consultation with a PCOS-specialist gynaecologist or endocrinologist today and take the first concrete step toward a personalised management plan that is built around you.
Frequently Asked Questions
Q: Can PCOS go away on its own after a certain age? PCOS does not disappear entirely, but many women experience a meaningful reduction in symptoms — particularly androgen-driven ones like acne and hirsutism — as they approach their 40s and perimenopause, due to a natural age-related decline in androgen production. However, the metabolic components of PCOS, including insulin resistance and cardiovascular risk, persist and require continued medical monitoring throughout life.
Q: Is it possible to have a healthy pregnancy with PCOS? Absolutely — the majority of women with PCOS do conceive and deliver healthy babies, though some may require support through ovulation induction medications, lifestyle modifications, or assisted reproductive technology. PCOS does increase the risk of gestational diabetes and other pregnancy complications, so specialist antenatal care and early glucose screening are strongly recommended.
Q: Does having PCOS mean I will definitely get diabetes? Having PCOS significantly increases your lifetime risk of developing type 2 diabetes compared to women without the condition — but it is not a certainty, and the risk is highly modifiable. Women who maintain an anti-inflammatory diet, exercise regularly, manage their weight, and monitor their blood glucose are able to meaningfully reduce or delay the onset of diabetes, even with a PCOS diagnosis.
Q: Can diet alone control PCOS without medication? For some women — particularly those with mild or early-stage PCOS — a well-structured low-glycemic, anti-inflammatory diet combined with regular exercise can produce significant symptom improvement without medication. However, many women with more pronounced insulin resistance, androgen excess, or fertility challenges require a combination of dietary changes and targeted medical treatment for optimal results, and there is no shame in needing medication alongside lifestyle changes.
Q: How do I know if my PCOS treatment is actually working? Effective PCOS management shows up in both subjective and objective improvements — more regular menstrual cycles, reduced acne or hair loss, improved energy levels, and a greater sense of wellbeing are meaningful clinical signs. Your doctor should also be monitoring objective markers including androgen levels, fasting glucose, insulin, HbA1c, and lipid panels at regular intervals, and meaningful improvement in these numbers confirms that your PCOS treatment plan is delivering real results.